
Regenerative Research Roundup – April 2026
- jtomkin3
- Apr 1
- 5 min read

Welcome to the Regenerative Research Roundup, where we look through recently published research and bring you the best of the best in a quick-to-read digest.
This month, we explore:
Overview effect of blood-draw volume on PRP efficacy in head-to-head studies with HA, CS and saline
The influence of tendon location and sex on clinical responses to PRP
Head-to-head of PRP and steroids for SIJ pain
Intradiscal PRP for discogenic low back pain and qMRI changes
Let’s dive in!
Autologous platelet-rich plasma versus hyaluronic acid, corticosteroids or saline for knee osteoarthritis: can blood draw volume serve as a proxy for platelet dose? A systematic review and meta-analysis
International Orthopaedics // LOE: I
PRIMSA reporting guideline for systematic review of RCTs comparing intra-articular PRP with HA, corticosteroid (CS), or saline placebo (NS) for symptomatic knee OA, with the goal of assessing whether blood-draw volume/platelet dose is associated with treatment effect. VAS pain and WOMAC function scores were measured at 6 and 12 months, and PRP subgroups were stratified by blood-draw volume (< 40 mL vs ≥ 40 mL).
Key Findings:
At 6 months, PRP improved VAS and WOMAC scores on par with HA and CS.
At 12 months, PRP displayed superior improvements in VAS and WOMAC scores compared to HA and CS.
In PRP vs HA trials, a blood draw volume greater than 40 mL was associated with larger improvements in 6-month WOMAC and 12-month VAS scores
Clinical Perspective:
After analyzing more than 62 clinical trials and measuring outcomes in 4,969 patients suffering from knee OA, it becomes abundantly clear that PRP blood-draw volume plays a significant role in successful outcomes. As consistently reported throughout the literature, platelet dose is most critical factor in patient response, with 10B platelets being the clinical threshold for knee OA. Blood draw volume becomes the simplest metric in which to assess whether a PRP system can provide an adequate dose.
As a point of care treatment, PRP’s efficacy relies directly on the raw materials being processed, with higher final doses corresponding to larger blood-draw volumes, resulting in better patient outcomes.
ACCESS HERE: https://doi.org/10.1007/s00264-026-06782-7
Influence of Tendon Location on the Clinical Response to Platelet-Rich Plasma: A Prospective Cohort Study of Rotator Cuff, Achilles and Patellar Tendinopathies
Journal of Clinical Medicine // LOE: III
This prospective observational study followed 49 tendinopathy patients (rotator cuff n=15, Achilles n=18, patellar n=16) treated with three “multitarget” PRP sessions (intratendinous + peritendinous) spaced 2 weeks apart. Outcomes were assessed at baseline and 6 months using tendon-specific scores (DASH, VISA-A, VISA-P) and responders were defined by MCII.
Key Findings:
The overall portion of responders at 6 months of treatment was 67.4%., with a significant improvement observed between baseline scores and the 6-month scores.
Responder rates differed by tendon: supraspinatus tendon of the rotator cuff (73.3%), achilles (75.0%), and patellar (50.0%).
Significant score improvement was seen for rotator cuff and achilles groups, but not for patellar tendinopathy group.
Response rates differed by sex: women had an overall response of 92.3% compared to 58.3% for men.
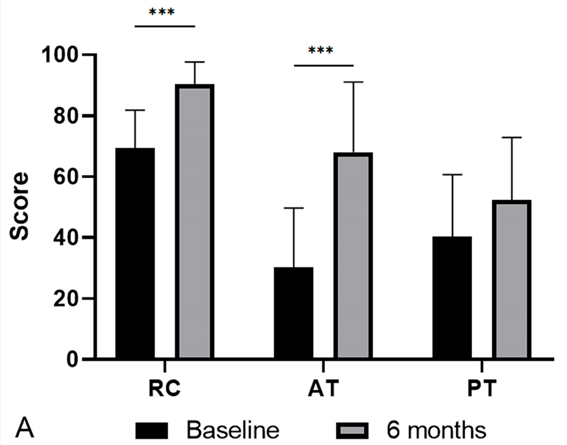
Figure 3. Clinical scores. Results of the scales before and after. The RC group was evaluated using the DASH scale, the AT group using the VISA-A scale, and the PT group using the VISA-P scale.
Clinical Perspective:
Although an interest topic of discussion, ultimately, no derivable conclusions can be made due to PRP protocol being inadequate for proper tissue stimulus. In favor of the authors, the PRP protocol is clearly outlined: consisting of a 48 mL blood draw, single-spin, LP-PRP, concentrated at ~2× baseline, delivered in an injection volume ranging between 8–12 mL universally and guided by ultrasound. Typical PRP injection volumes for the Achilles tendon range between 2-4 mL and injecting 8-12 mL is not only going to dilute down your platelet concentration to being insufficient to a trigger a meaningful biological effect but also be extremely painful for the patient as they intaking loads of volume pressure into a small area.
It goes the show that with proper preparation system, allowing to concentrate platelets at lower injection volumes would be derive higher response rates among patients, but also reduce pain during the injection itself.
ACCESS HERE: https://doi.org/10.3390/jcm15052005
Comparison of CT-guided platelet-rich plasma versus steroid/anesthetic injection for treatment of sacroiliac joint pain: a randomized, single-blinded, controlled trial
American Journal of Neuroradiology // LOE: I
This single-blinded RCT enrolled 44 adults with chronic sacroiliac joint (SIJ) pain confirmed by ≥50% relief after anesthetic block, then randomized patients to CT-guided PRP vs steroid/anesthetic injection with outcomes measured over 3 months. Primary outcome was measured via change in numeric rating scale (NRS) pain scores, secondary outcomes included disability and quality-of-life metrics.
Key Findings:
Both groups treatment arms displayed significant pain reduction at 3 months
The steroid/anaesthetic injection treatment group produced greater early pain relief favored steroid/anesthetic injection, while PRP demonstrated greater sustained improvement
The PRP treatment group displayed non-significant trend towards higher responder rates and favorable physical quality of life outcomes at 3 months
Clinical Perspective:
This study tackles one of the largest dilemmas encountered in the MSK and Pain Management space, short-term pain relief versus slow onset, yet durable benefit. According to the Clinical Trials protocol PDF, they used the Cascade Autologous Platelet system, drawing 20 mL of blood, concentrating down to 3-5cc PRP via dual-spin and activating platelets with calcium chloride before injecting. Although the data presented does trend in favor of PRP usage for sustained, one of the study limitations is how weak the PRP protocol and system is. With a 20 mL blood draw even at highly concentrated and efficient dual-spin system, the platelet dose is insufficient to achieve meaningful clinical results leading to no significant conclusions to be drawn.
ACCESS HERE: https://doi.org/10.3174/ajnr.A9307
Intradiscal platelet-rich plasma for discogenic low back pain: a prospective cohort study of early clinical outcomes and quantitative MRI findings
Scientific Reports // LOE: III
This prospective single-arm cohort study evaluated intradiscal PRP for discogenic low back pain with outcomes assessed at baseline, 1, 3, and 6 months, alongside quantitative MRI measures (whole-disc T2 and adjacent vertebral marrow fat fraction). 45 patients were recruited and 29 completed follow-ups.
Key Findings:
Pain and function improved over time: VAS, ODI, and FRI all decreased significantly at 6 months
The composite responder rate at 6 months was 79.3% with responders having achieved ≥30% reduction in both VAS and ODI scores.
Adjacent vertebral marrow fat fraction declined significantly overtime and correlated with symptom improvements.
Clinical Perspective:
In this study, intradiscal PRP was prepared using the Arthrex ACP double-syringe protocol, consisting of a single low-speed spin, LP-PRP with a 2 mL injection volume per disc – effectively delivering a low platelet dose at concentrations ranging from 2-3x baseline. According to Lutz et al. and the overall literature, intradiscal PRP injections require concentration of 10x baseline to receive meaningful outcomes, measured across the Functional Rating Index and NASS Patient Satisfaction Index.
Although reduction qMRI displayed structural improvements and reduction in VAS and ODI scores were observed, using a higher-concentrated PRP system would infer stronger clinical results.
ACCESS HERE: https://doi.org/10.1038/s41598-026-42909-x
Comments